Serratus anterior muscle
- Anatomy
- Kinesiology
- Fascial Connection
- Pathomechanics
- Strength tests
- Muscle palpation
- Common Trigger Point Location and Referral Pattern
- Trigger point therapy
- Dry Needling Therapy
- How to strengthen serratus anterior
Anatomy
Serratus anterior origin
The serratus anterior muscle originates from the outer surfaces and superior borders of the first to eighth or nine ribs and also from the fascia covering the intervening intercostal muscles
Serratus anterior insertion
The serratus anterior muscle inserts onto the anterior aspect of the medial border of the scapula, with the heaviest attachment onto its inferior angle.
- One digitation from the superior angle to the root of spine,
- Two digitations to the medial border, and
- Five digitations to the inferior angle.
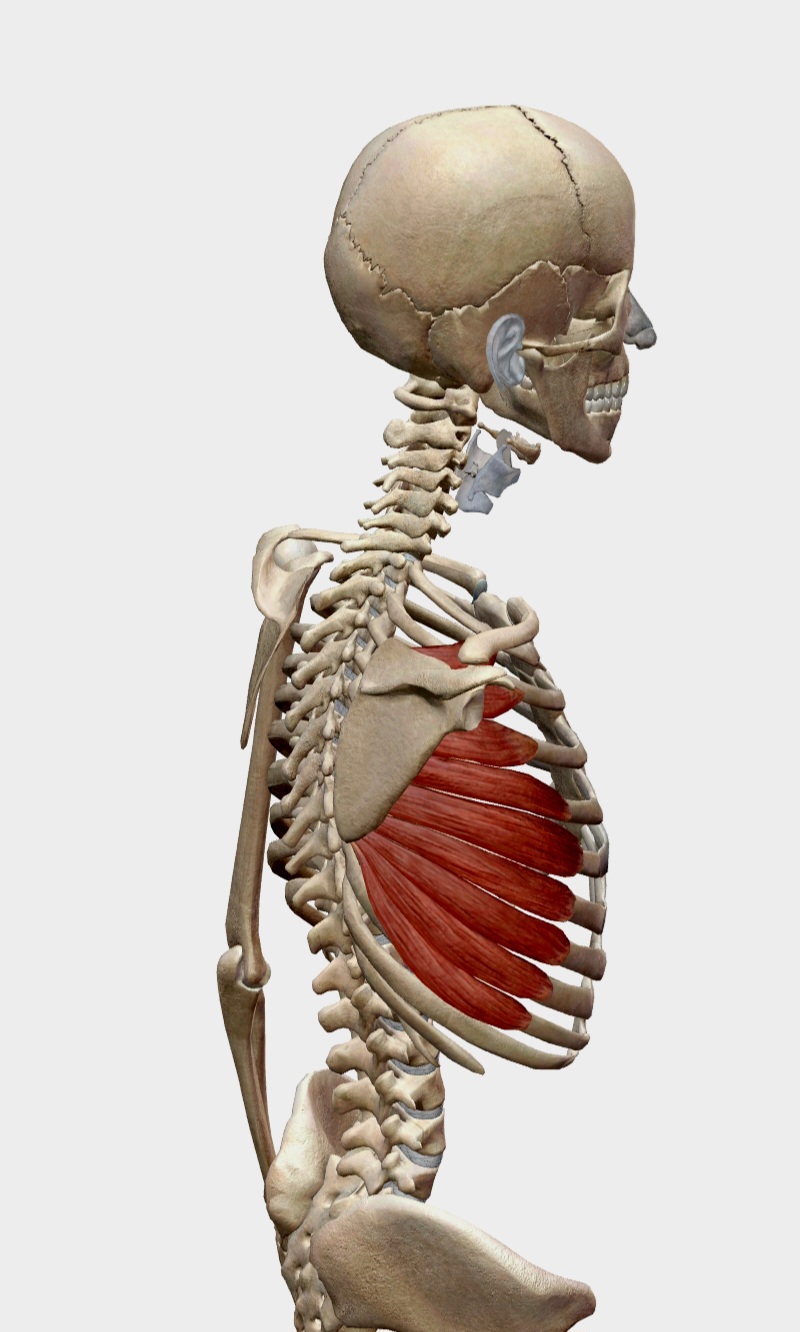
Serratus anterior muscle anatomy
Nerves
The long thoracic nerve (C5, C6, and C7) innervates the serratus anterior muscle. The weakness of the serratus anterior muscle can be caused by compression or inflammation of the long thoracic nerve due to traumatic event or overuse.
Arteries
The lateral thoracic artery and the thoracodorsal artery supply blood to the serratus anterior.
Kinesiology
The action of the serratus anterior muscle includes:
- Protraction of the scapula
- Upward rotation of the scapula
- Posterior tilting/tipping of scapula during arm elevation
- Stabilization of the scapula.
Fascial Connection
The serratus anterior muscle is interconnected with the rhomboid and ipsilateral external oblique muscles. The external oblique connects with the contralateral internal oblique and the adductors. This connectivity is crucial for horizontal force production, akin to the serape effect, which enhances the efficiency and coordination of movements such as punching or throwing. The serratus anterior also plays a significant role in scapular protraction and stabilization, essential for optimal shoulder function and injury prevention. Proper engagement and strength of this muscle can improve posture, reduce the risk of shoulder impingements, and enhance overall athletic performance.
Pathomechanics
Weakness of the serratus anterior due to long thoracic nerve injury can lead to a loss of scapular stability during shoulder abduction, which may manifest as scapular winging. This weakness also results in a loss of upward rotation and posterior tilting of the scapula, causing impingement of subacromial contents such as the supraspinatus tendon. Overall, this leads to shoulder pain and dysfunction due to scapular dyskinesis.
The scapular dyskinesis is commonly associated with forward head posture and rounded shoulder.
Weakness of the serratus anterior muscle
|Loss of scapular stability during arm movements.
|Scapular dyskinesis / Scapular winging
|Synergistic overactivation of upper and lower trapezius.
|Loss of space clearance in subacromial space during overhead activities / Change in line of pull of rotator cuff muscles.
|Impingement of subacromial contents (e.g. Supraspinatus tendon or subacromial bursae) / Rotator cuff injuries.
Strength tests
Shoulder Abduction Test
To test the strength of the serratus anterior muscle, have the patient seated in a chair. Ask the patient to abduct or flex the shoulder to 120 degrees. The therapist should place one hand on the outer border of the scapula and the other hand on the humerus, then resist the motion isometrically. Weakness of the serratus anterior can be observed if the scapula fails to produce significant upward rotation force against the examiner's hand.
Protraction Test
This test can be performed with the patient either sitting or supine, with the shoulder flexed to about 90 degrees and the elbow fully extended. The examiner then pushes the scapula into a position of retraction and internal rotation. In the case of serratus anterior weakness, the medial border of the scapula will flare up.
Muscle palpation
With the patient in a sidelying position and the shoulder abducted, the therapist can easily access the mid-axillary line. Starting at the level of the nipple, the therapist palpates the 5th and 6th ribs, then moves downward to the 9th rib and upward to the 1st rib slips.
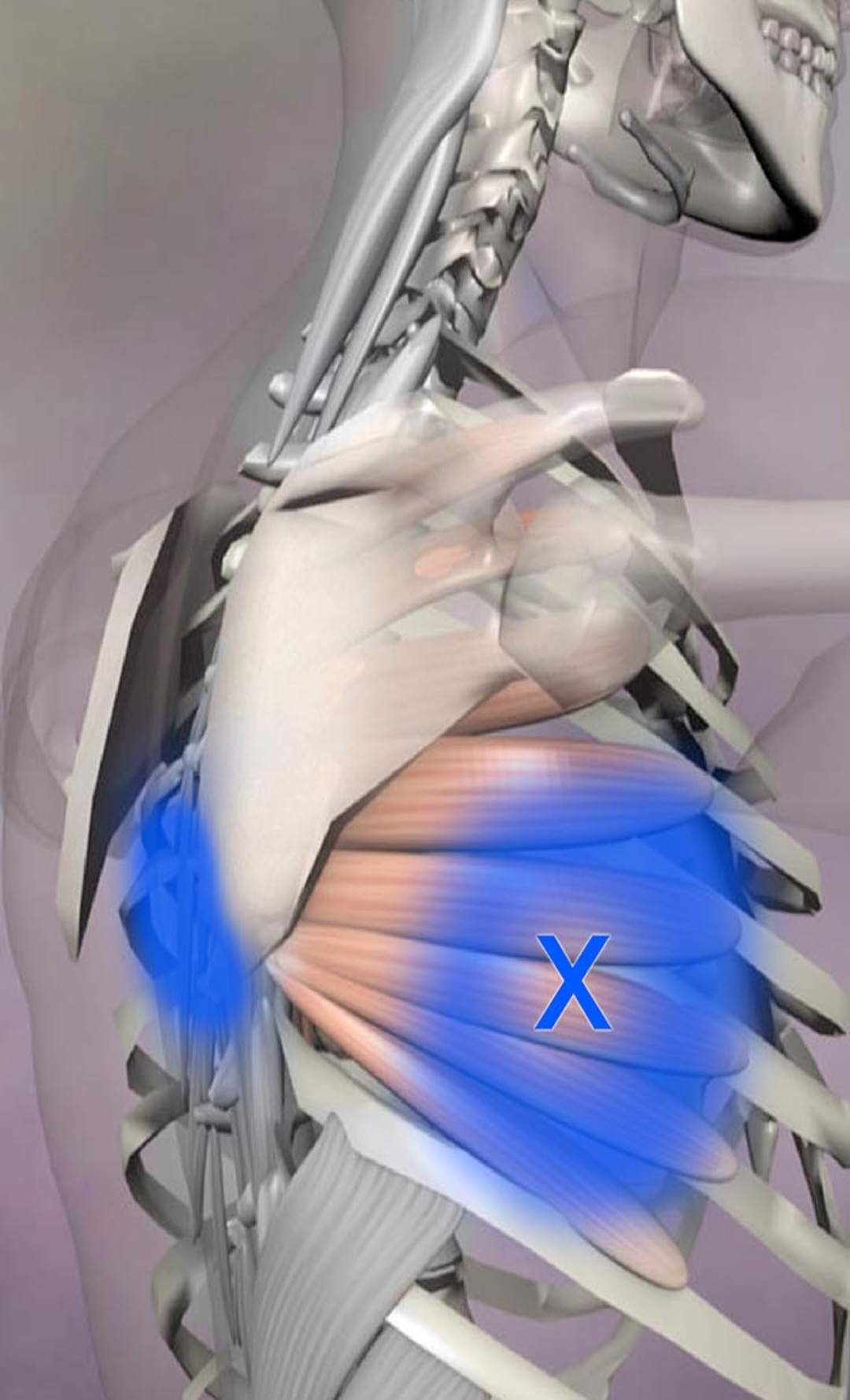
Common Trigger Point Location and Referral Pattern
Trigger Points
Common trigger points in the serratus anterior are located along the muscle, particularly in the mid-axillary line (along the side of the rib cage) at the level of ribs 5 and 6.
Referral Pattern
Pain from serratus anterior trigger points can refer to the side and back of the chest, down the arm, and to the medial border of the scapula, especially at the medial to the inferior angle of the scapula. It may mimic angina or be confused with issues related to the heart, shoulder, or upper back.

Sattelilite trigger points
- Pectoralis major
- SCM
- Scalenus medius
- Trapezius
- Rhomboids
- Diaphragm
- External oblique
Causes/Perpetuating factors
- Severe prolonged coughing
- Overuse in sports (e.g. tennis, swimming, boxing, pullups and pushups.)
- Lifting heavy objects
- Anxiety
Trigger point therapy
Involves applying direct pressure to the trigger points to deactivate them. Techniques may include:
- Sustained pressure: Using fingers, thumbs, or tools to apply steady pressure to the trigger point until it releases.
- Myofascial release: Gentle, sustained pressure to elongate and relax the fascia.
- Stretching: Incorporating gentle stretches after trigger point release to help maintain muscle flexibility.
Dry Needling Therapy
Position the patient in a sidelying position with the side to be treated facing upward and the arm resting in front. Secure the trigger point over a rib by passively moving the arm, placing the index and middle fingers' distal phalangeal joints in the intercostal spaces above and below the trigger point. Insert the needle perpendicular to the skin between the distal phalangeal joints, angling it tangentially toward the trigger point while staying over the rib. Alternatively, the muscle can also be needled from the medial aspect of the scapula, similar to the technique used for the subscapularis muscle.
How to strengthen serratus anterior
The important serratus anterior muscle exercises include:
- Knee pushup plus - on stable surface
- Pushup plus - on stable surface
- Pushup plus - on unstable, oscillating unstable surface
- TRX push plus
- Dynamic hug
- Serratus punches
- Turish getup
- Scaption
- Towel wall slides
- Forward punch plus - ipsilateral closed chain leg extension
- Forward punch plus - open chain serappe effect
- Plyo pushups
- Med ball SA throw
- Medicine ball rotational wall toss.
Start in a knee push-up position (on your hands and knees). Push your shoulder blades forward to engage your serratus anterior muscle.
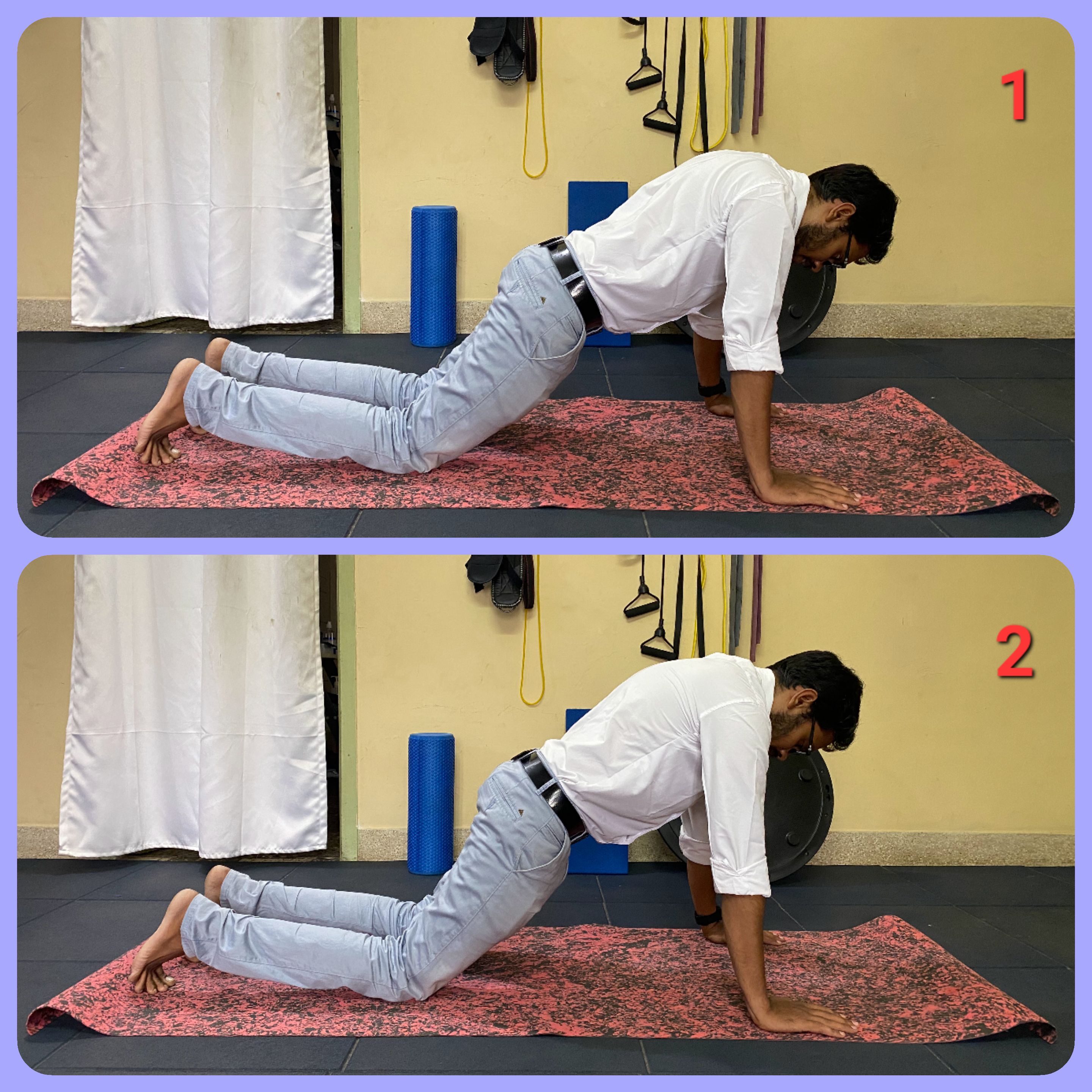
Knee push plus exercise for serratus anterior
Begin in a regular push-up position. As you push up, move your shoulder blades forward to activate your serratus anterior muscle.
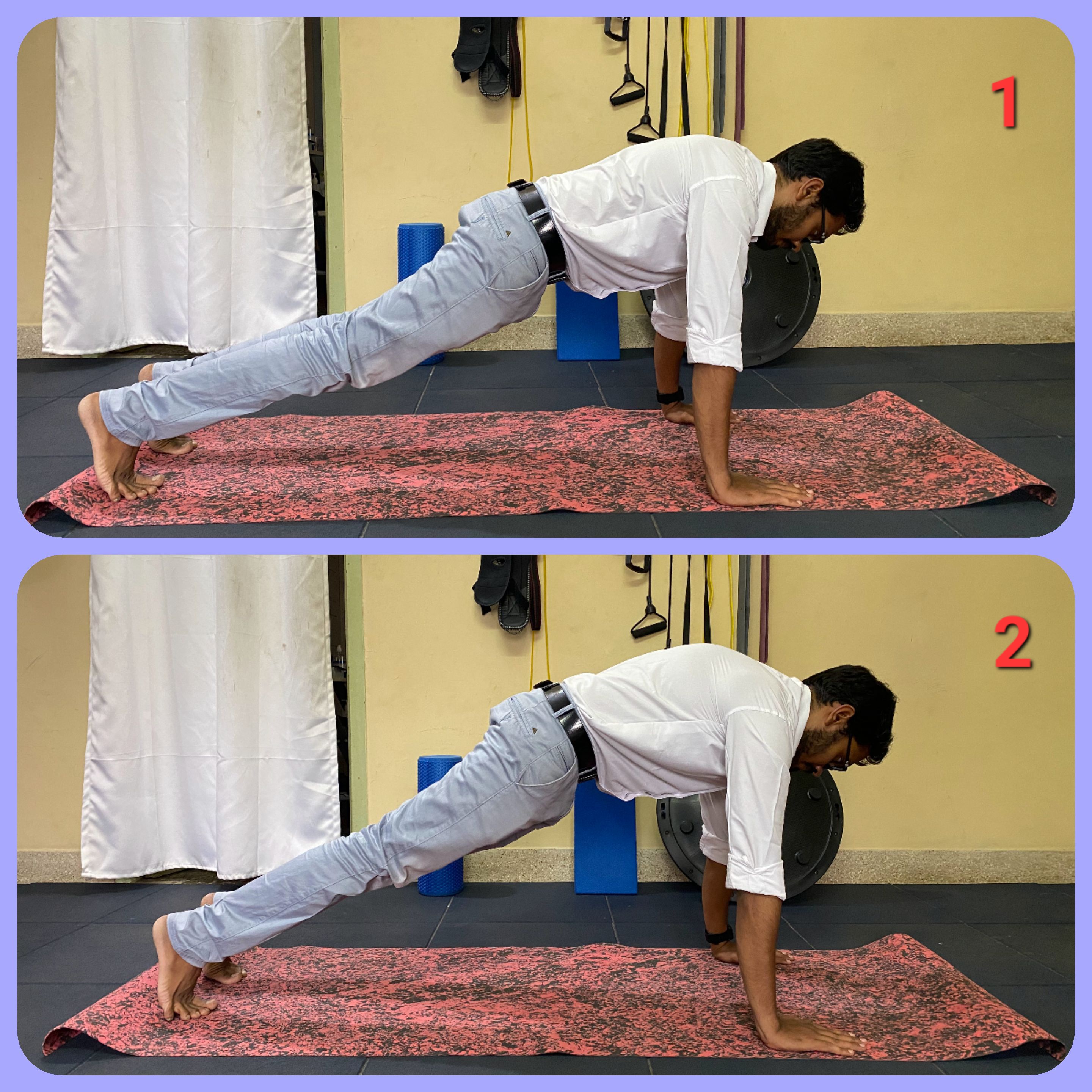
Pushup plus exercise for serratus anterior
Start in a regular push-up position with your hands on a BOSU ball. Push your shoulder blades forward to engage your serratus anterior muscle. To progress, have a therapist oscillate the BOSU ball while you perform the push-up plus, activating the serratus anterior on an unstable surface.
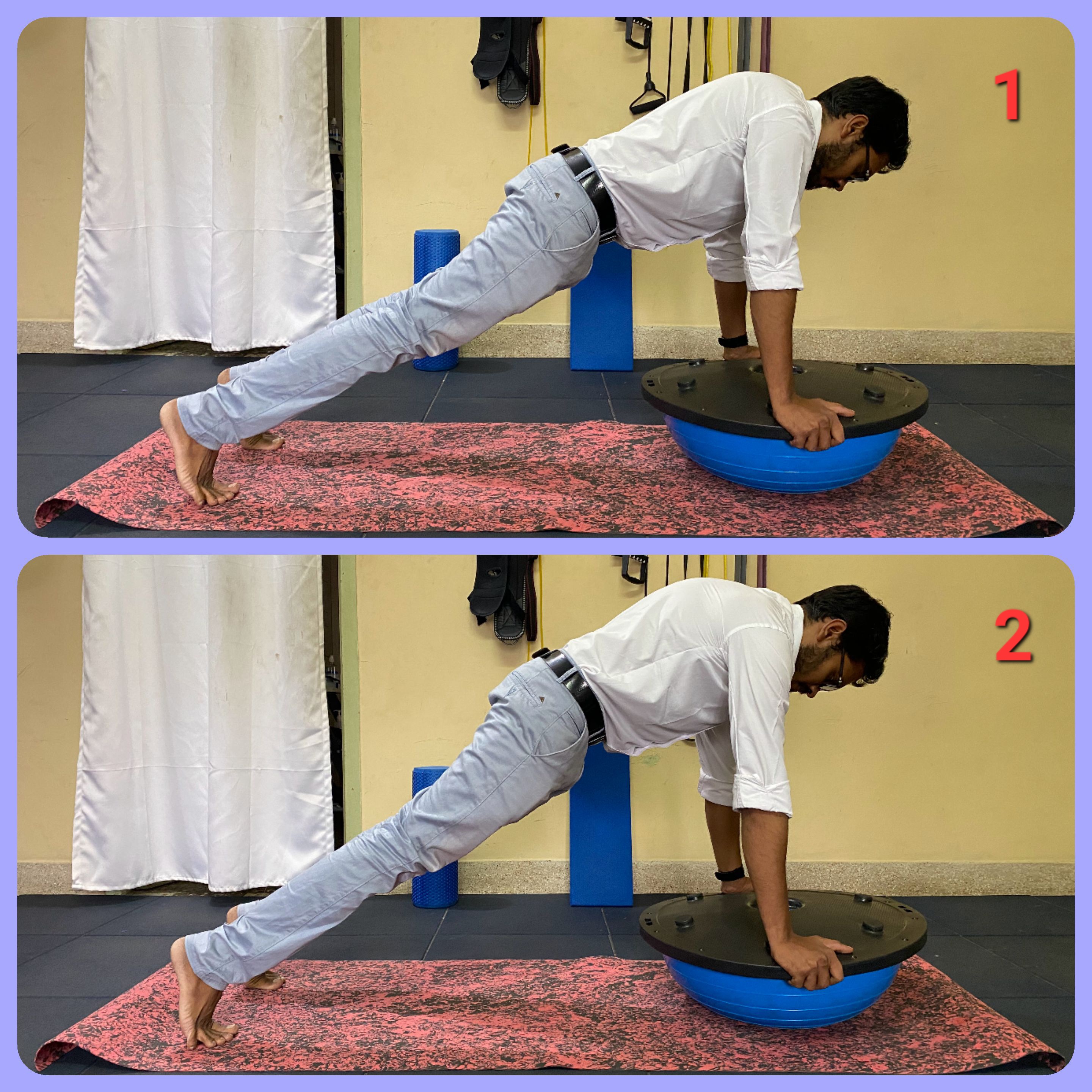
Pushup plus exercise for serratus anterior on unstable or oscillating unstable surface
Position the TRX ropes at knee level. Hold onto the TRX handles and perform a forward punching motion to activate the serratus anterior muscle.

Serratus anterior pushup plus exercise on TRX
Using a theraband or resistance tube, place the middle of the band behind your upper back. Hold the band with your hands below shoulder level, flexed at about 60 degrees. Perform a hugging motion, pushing your shoulder blades forward to engage the serratus anterior muscle.

Dynamic hug exercise for serratus anterior
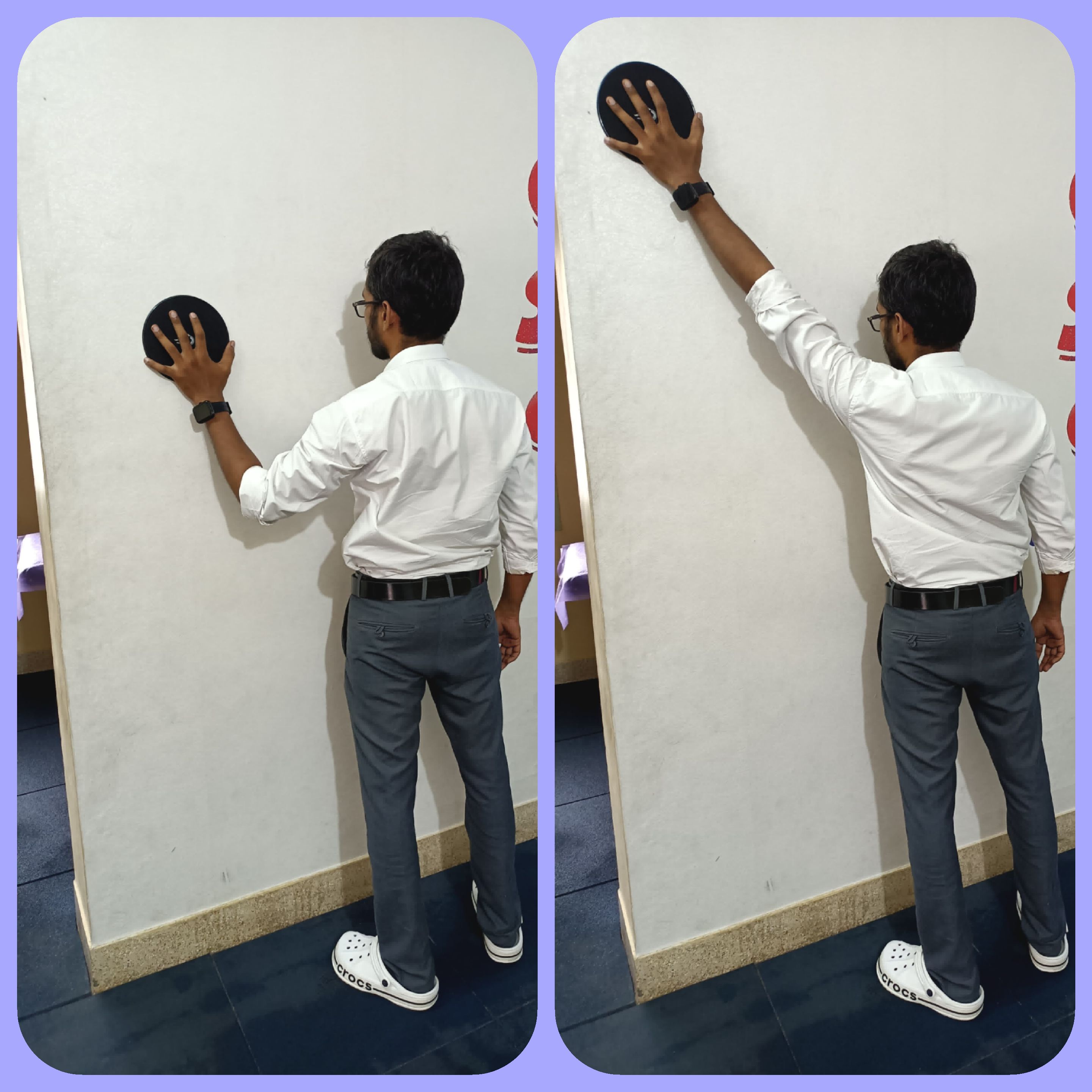
This basic-level exercise effectively activates the serratus anterior muscle. Place a Swiss ball against a wall and press it forward at shoulder level. Push your shoulder blades forward to engage the serratus anterior muscle. Start with isometric holds and gradually increase repetitions for isotonic movement progression.

Serratus punches exercise
The Turkish Get-Up is a complex full-body exercise that involves transitioning from lying down to standing while holding a weight overhead. It requires coordination, stability, and strength throughout the body, making it a challenging yet effective exercise for improving core strength, shoulder stability, and overall mobility. Its integrated nature activates muscles including the serratus anterior, contributing to enhanced functional fitness.

Turkish getup exercise for serratus anterior
Perform this exercise by holding a dumbbell in both hands and lifting it to 90 degrees in the horizontal plane. Hold this position for 10 seconds and repeat 10 times. This movement activates the serratus anterior muscles while promoting upward rotation of the scapula.

Scaption exercise for serratus anterior
To perform the wall slide exercise, stand with a towel or sliding board against the wall. Slide your arms diagonally upwards along the wall, maintaining contact with the towel or board. This movement helps activate muscles like the serratus anterior and promotes shoulder mobility and stability.
Wall slide exercise for serratus anterior
Stand in a split stance with the opposite-side hip extended forward. Hold a theraband or functional trainer handle and push it forward. This position activates the serratus anterior along with the anterior oblique chain, enhancing core stability and functional movement integration.

Ipsilateral closed chain serratus anterior punches
Perform this exercise with one leg lifted off the ground, creating a serrape effect while executing a forward punch motion. This engages the serratus anterior muscle dynamically, emphasizing shoulder stability and core activation in an open chain movement pattern.

Serratus anterior punches with serappe effect
To perform a plyometric push-up, start in a push-up position. Lower your body towards the ground in a controlled manner, then explosively push off the ground so that your hands leave the ground briefly. This exercise activates the serratus anterior muscle explosively, enhancing upper body power and strength.

Plyo pushups for serratus anterior

Medicine ball throw for serratus anterior

Rotational medicine ball throw for serratus anterior
-
Anatomy and Physiology
- Moore, K. L., Dalley, A. F., & Agur, A. M. (2013). Clinically Oriented Anatomy. Wolters Kluwer Health/Lippincott Williams & Wilkins.
- Drake, R. L., Vogl, A. W., & Mitchell, A. W. M. (2014). Gray's Anatomy for Students. Elsevier Health Sciences.
-
Posture and Ergonomics
- Kendall, F. P., McCreary, E. K., & Provance, P. G. (2005). Muscles: Testing and Function, with Posture and Pain. Lippincott Williams & Wilkins.
- Neumann, D. A. (2017). Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation. Elsevier Health Sciences.
-
Kinesiology and Function
- Sahrmann, S. A. (2002). Diagnosis and Treatment of Movement Impairment Syndromes. Mosby.
- Ludewig, P. M., & Reynolds, J. F. (2009). The association of scapular kinematics and glenohumeral joint pathologies. Journal of Orthopaedic & Sports Physical Therapy, 39(2), 90-104.
-
Pathomechanics and Clinical Implications
- Kibler, W. B., & Sciascia, A. (2010). Current concepts: scapular dyskinesis. British Journal of Sports Medicine, 44(5), 300-305.
- Wadsworth, D. J., & Bullock-Saxton, J. E. (1997). Recruitment patterns of the scapular rotator muscles in freestyle swimmers with subacromial impingement. International Journal of Sports Medicine, 18(8), 618-624.
-
Assessment and Testing
- Magee, D. J. (2014). Orthopedic Physical Assessment. Elsevier Health Sciences.
- Clarkson, H. M. (2013). Musculoskeletal Assessment: Joint Range of Motion and Manual Muscle Strength. Lippincott Williams & Wilkins.
-
Trigger Points and Myofascial Pain
- Travell, J. G., & Simons, D. G. (1999). Myofascial Pain and Dysfunction: The Trigger Point Manual. Lippincott Williams & Wilkins.
- Dommerholt, J., & Fernández-de-Las-Peñas, C. (2013). Trigger Point Dry Needling: An Evidence and Clinical-Based Approach. Elsevier Health Sciences.
-
Dry Needling Techniques
- Simons, D. G., Travell, J. G., & Simons, L. S. (1999). Myofascial Pain and Dysfunction: The Trigger Point Manual, Vol. 1. Lippincott Williams & Wilkins.
- Ma, Y. T., & Cho, Z. H. (2004). Biomedical Acupuncture for Pain Management: An Integrative Approach. Elsevier Health Sciences.
-
Exercises for Serratus Anterior
- Cools, A. M., Dewitte, V., Lanszweert, F., Notebaert, D., Roets, A., Soetens, B., ... & Witvrouw, E. E. (2007). Rehabilitation of scapular muscle balance: which exercises to prescribe? The American Journal of Sports Medicine, 35(10), 1744-1751.
- McDonnell, M. K., Sahrmann, S. A., & Van Dillen, L. R. (2005). A specific exercise program and modification of postural alignment for treatment of cervicogenic headache: a case report. Journal of Orthopaedic & Sports Physical Therapy, 35(1), 3-15.
| Name | : | Deva senathipathi |
| Qualifications | : | Physiotherapist |





