Diabetes mellitus
Diabetes mellitus is a chronic progressive metabolic disease characterized by impaired carbohydrate metabolism in the body leading to hyperglycemia (Increased blood sugar level).
Physiology of Blood Glucose Regulations
Action of Insulin
-
Food intake
|
Absorption of glucose in small intestine
|
Increased blood glucose level (Hyperglycemia)
|
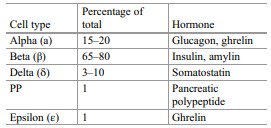
Release of Insulin from the Beta cells of pancrease
|
Insulin stimulates receptors in Liver and muscles
|
Increased glucose uptake by the liver and muscles
|
Stored as Glycogen
|
Reduced blood glucose level to Normal level
Action of Glucogon
-
Intense exercise / deep brain work
|
Reduced blood glucose level (Hypoglycemia)
|
Increased hunger stimulus from the brain
|
Release of Glucogon from the Alpha cells of pancrease
|
Stimulates liver to causes glucogenolysis
|
Release of glucose from Glycogens
|
Increased blood glucose to Normal level.
Classification
- Type 1 diabetes
- Type 2 diabetes
- Gestational diabetes
- Other types
- Maturity onset diabetes of the young (MODY)
- Neonatal diabetes
- Wolfram Syndrome
- Alström Syndrome
- Latent Autoimmune diabetes in Adults (LADA)
- Type 3c diabetes
- Steroid-induced diabetes
- Cystic fibrosis diabetes
Type I Diabetes Mellitus
It is an autoimmune disorder (familial influence) leads to the distruction of pancreatic beta cells results in low level of insulin. Common in children and yound adults. It occurs before 30 years of age with incidence of 10 %.
It is also called as insulin dependent diabetes mellitus or Juvenile diabetes mellitus.
Risk factor
- Younger adults/children
- Family history
Pathophysiology
Destruction of Beta cells of pancrease due to increased pancreatic antibodies (i.e. IAA)|
Insulin deficiency
|
Reduced glucose utilization
|
Hyperglycemia
Type II Diabetes Mellitus
Type II DM characterized by increased insulin resistance and reduced insulin production due to inactivity. It is most common type accounts in 90% of cases and usually occurs after 35 years of age.
Risk factors
| Modifiable | Non modifiable |
|---|---|
| Pre-diabetes CVD Hypertension Low HDL High Triglycerides Obesity PCOS Physical inactivity |
Age: > 35 Race: African american, Asian american, Hispanic or Latino Family History. |
Pathophysiology
Sedentary lifestyle/physically inactive/obesity|
Increased carbohydrate intake
|
Increased insulin resistance
|
Increased workload of beta cells of pancrease to produce more insulin
|
Beta cells failure
|
Reduced insulin production
|
Reduced glucose utilization by the cells
|
Hyperglycemia
Gestational Diabetes Mellitus
Increased maternal blood glucose during pregnancy. GDM resolves after giving birth. but, in some cases it leads to Type II DM.
Risk factors
- GDM during previous pregnancy
- Overweight
- Family history
- PCOS
Pathophysiology
Increased placental hormones during 2nd & 3rd trimester|
Increased insulin resistance for mother
|
Increased maternal blood glucose, amino acids & lipids
|
Hyperglycemia (Normal process for providing nutrients to growing fetus)
Clinical Features of Diabetes mellitus
- Fatigue
- Weight loss
- Polydipsia
- Polyuria
- Polyphagia
- Numbness & Tingling of extremities
- Blurred vision
- Intrinsic muscle wasting
- Charcot joints
- Diabetic foot ulceration
- Neurogenic bladder
- Gastroparesis
Investigations
1. Ketonuria
2. Proteinuria
3. Blood glucose
| Type | Fasting Glucose | Postprantial (After 2hours of meals) | HbA1C |
|---|---|---|---|
| Normal | 70-100mg/dl | 70-140mg/dl | > 5.6 |
| Prediabetes | 101-125mg/dl | 141-200mg/dl | 5.7 to 6.4 |
| Diabetes | >125mg/dl | >200mg/dl | > 6.5 |
4. Antibody test (Type I DM)
- ICA
- IAA
- GADA
- IA-2A
- ZnT8A
Treatments
Pharmacological
- Oral hypoglycemic agents
- Sulfonylureas (glipizide, glyburide, gliclazide, glimepiride)
- Meglitinides (repaglinide and nateglinide)
- Biguanides (metformin)
- Thiazolidinediones (rosiglitazone, pioglitazone)
- α-Glucosidase inhibitors (acarbose, miglitol, voglibose)
- DPP-4 inhibitors (sitagliptin, saxagliptin, vildagliptin, linagliptin, alogliptin)
- SGLT2 inhibitors (dapagliflozin and canagliflozin)
- Cycloset (bromocriptine)
Diet
- Balanced diet
- Low carb diet
- High protein diet
Exercise
- Brisk walking
- Aerobic dancing
- Resistance training
SHARE:


- Leonid Poretsky, Principles of Diabetes Mellitus.
- https://www.ncbi.nlm.nih.gov/books/NBK482386/
| Name | : | Deva senathipathi |
| Qualifications | : | Physiotherapist |





